Managing the pain associated with Osteonecrosis (Avascular Necrosis) is just as important as managing the disease. Remember, you know better than anyone else what level of pain you can deal with while trying to live a fully functioning life.
I’ve been on pain killers for about 16 months now. For the first few months I was on Oxycontin 7.5mg three times a day. Then I started taking Tramadol during the day and instead only took Oxycontin at night.
One of the problems with being on drugs like Oxycontin or Tramadol is that several doctors scared me and implied I could become addicted to pain killers. I know that taking pain killers is a risk. I am so overly self-aware about the possible physical and mental dependency risks that they are on my mind every time I take a pill. I know why doctors try to frighten their patients. Many people do abuse Oxycontin. However, it is very easy for a doctor to judge you when they haven’t lived with a disease like ON(AVN) that causes chronic pain.
During the holiday season, about a month ago, I decided to do two stupid things. First of all I abruptly stopped taking pain killers at night. Secondly, I decided to spend a day with my husband doing what an average 35-year-old would be doing. I went downtown on public transport with just my cane. I walked around, looked at the lights, went shopping at several stores, and spent a lot of time standing. By the time my husband and I went to dinner I was in so much pain I had to rest my legs on his lap. After dinner I could barely walk out of the restaurant and we had to get a cab back home. At home I couldn’t walk to the bathroom to brush my teeth. By the next morning I woke up in so much pain I spent the day on the couch without being able to leave the apartment.
In retrospect I was probably punishing my body, punishing it for not allowing me to lead a ‘normal’ life. I was also listening to all those voices in my head that kept saying, “you’ve been on pain killers for 16 months isn’t is time you got off of them and accept the pain!”. I kept replaying conversations I had with doctors who scared me into thinking I was going to become a drug addict.
The problem is that the level of pain associated with my osteonecrosis isn’t an acceptable level of pain. It isn’t a level of pain that allows me to do any of the things I need to do to work towards getting better such as swimming, physical therapy or walking up the three flights of stairs to my apartment. Choosing to stop taking pain killers at night and pushing myself were very foolish actions. It took me over a week before I could get my pain under control again.
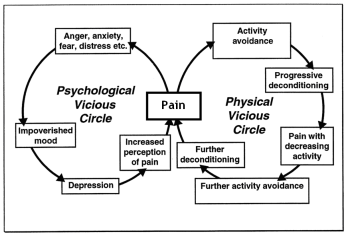
I would love nothing more than to wake up and live a full day without the aid of something to help me function. However, along with pain comes depression. Depression takes you to a place it’s hard to dig yourself out of. My mind becomes dark and I can’t get away from a cyclical obsessive pattern of thinking that I will never be able to live a full happy life again. Sometimes it makes me feel like I don’t want to live my life anymore. With ON(AVN) you are already grieving the loss of so many things, compounded with the pain, sometimes you feel like you are drowining in your disease. Osteonecrosis changes your life.
I went back to my primary care physician, we had a conversation about my pain and I decided to take Tramadol at night and to only take Oxycontin for break through pain. I was happy with this decision. I still have good pain days and bad pain days. Some days I deal with my grief better than other days, but one of the most important things I have noticed is how imperative it is to have good pain management.